If you are researching full arch dental implant treatment, you have very likely come across the terms All-On-4 and All-On-X. Both describe approaches to replacing an entire arch of teeth using implants and a fixed bridge, but they are not the same thing, and the differences between them are clinically meaningful.
This guide explains what each approach involves, how the two differ, what those differences mean for the final result, and how a treating dentist determines which option is appropriate for a given patient. It also introduces the concept of prosthetic classification, which plays an important role in understanding why the number of implants used can affect the type of bridge that is possible and the appearance of the final restoration.
This article is intended as educational background reading. Every patient’s anatomy, bone structure, and clinical situation is different. A thorough clinical assessment is the only reliable basis for determining which treatment approach is appropriate in any individual case.
What Is All-On-4?
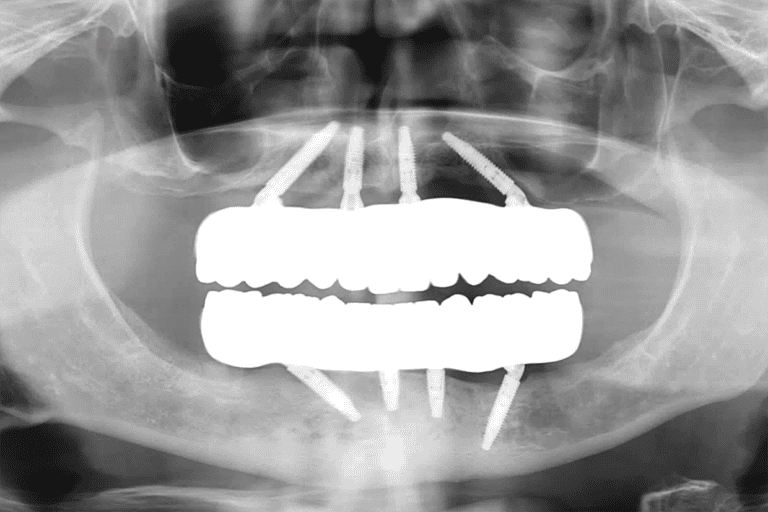
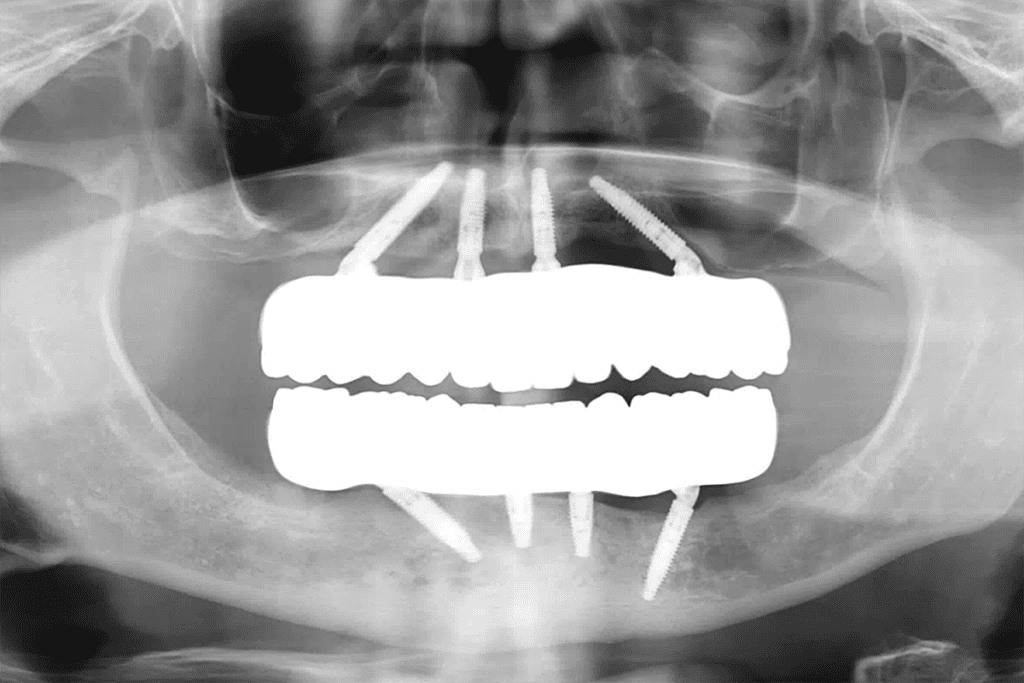
All-On-4 is a full arch implant protocol in which four dental implants are placed in the jawbone to support a fixed prosthetic bridge that replaces all of the teeth in that arch. The term refers specifically to the fixed use of four implants.
Two implants are placed vertically at the front of the jaw, and two are placed at an angle toward the rear. The angled placement of the posterior implants is a deliberate clinical technique designed to maximise contact with available bone and allow the bridge to extend further back in the mouth without requiring additional implants.
The All-On-4 protocol was developed to offer a fixed, implant-supported solution for patients with significant tooth loss, including those who may not have sufficient bone volume in the rear of the jaw to support implants in those positions. By tilting the posterior implants, the protocol can often be completed without bone grafting, though this depends on the individual patient’s bone structure.
What Is All-On-X?
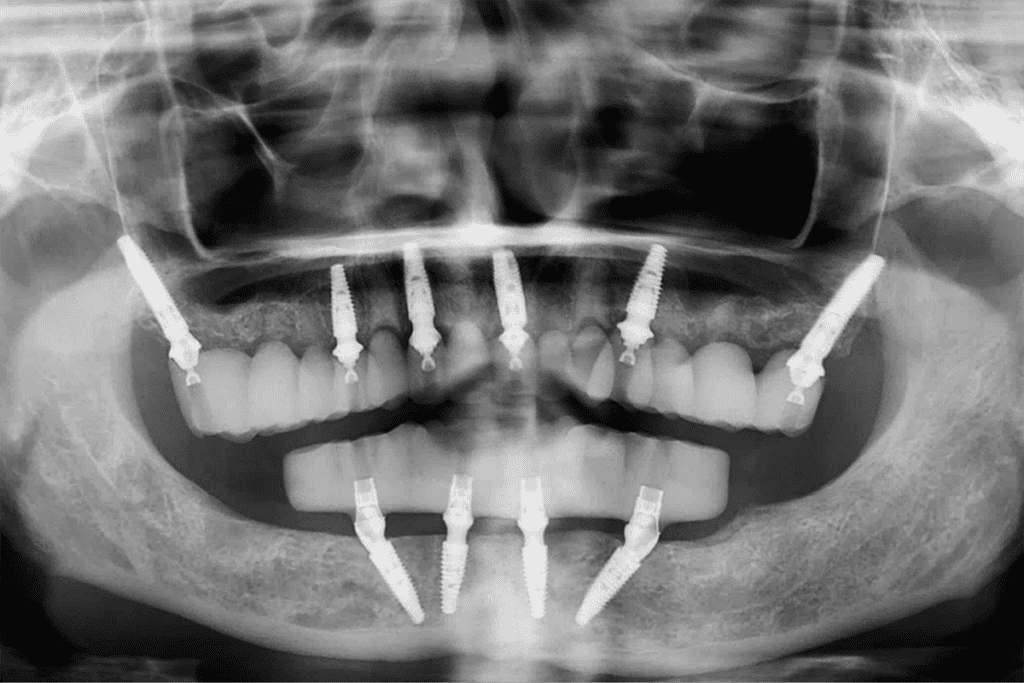
All-On-X is a broader term describing full arch implant treatment in which the number of implants used is not fixed at four. The X represents a variable number, typically six or more implants per arch, determined by the patient’s individual clinical requirements rather than a standardised protocol.
The rationale for using more than four implants in a full arch case relates to the distribution of load across the jawbone, the degree of support available to the prosthetic bridge, and the clinical goals of the treating dentist and patient. In certain cases, particularly those involving specific prosthetic outcomes or patients with particular bone anatomy, additional implants may be clinically indicated to achieve the desired result.
Each implant placed in the jawbone acts as an anchor point for the prosthetic bridge. A greater number of anchor points distributes the forces of biting and chewing across a wider area of bone. This has implications for long-term bone preservation, prosthetic stability, and the type of bridge design that is achievable.
FP1 and FP3: Understanding Prosthetic Bridge Classifications
One of the most important but least widely explained aspects of full arch implant treatment is the classification of the prosthetic bridge itself. In implant dentistry, fixed prostheses are classified using a system that describes what the bridge replaces and how it sits in relation to the gum tissue. The two classifications most relevant to All-On-4 and All-On-X cases are FP1 and FP3.
FP3: Replacing Teeth and Gum Tissue
An FP3 prosthesis replaces both the crowns of the teeth and a portion of the gum tissue. In practical terms, this means the bridge includes pink acrylic or ceramic material that visually recreates the appearance of gum tissue above the teeth.
FP3 bridges are the traditional prosthetic format associated with All-On-4 treatment. They are a well-established option and produce functional, aesthetic results for a wide range of patients. The inclusion of simulated gum tissue in the bridge design means that the exact volume and contour of the patient’s natural gum line is less critical to the final aesthetic, which can make treatment planning more straightforward in certain cases.
FP1: A Direct-to-Gum Bridge Design
An FP1 prosthesis takes a fundamentally different approach. Rather than incorporating simulated gum tissue into the bridge itself, an FP1 bridge attaches directly to the gum line. The gum tissue is surgically shaped and scalloped during treatment so that it closely follows the contour of the individual teeth in the bridge design.
The result is a prosthesis in which the teeth appear to emerge directly from the gum tissue, in a way that closely resembles the appearance of natural dentition. There is no visible pink material above the teeth. For patients who are suited to this approach, it can produce a result that is more difficult to distinguish from natural teeth at conversational distances.
Achieving a well-executed FP1 result requires a specific set of clinical conditions. The gum tissue must be of sufficient volume and quality to be shaped and maintained in the desired contour. The prosthetic bridge must be supported with a level of stability and precision that allows it to sit flush with the sculpted gum tissue without visible gaps or inconsistencies. These requirements have direct implications for how many implants are appropriate to use.

FP1 vs FP3 at a Glance
| FP3 | FP1 |
| Bridge includes simulated gum-coloured material | Bridge attaches directly to the natural gum line, which is surgically shaped to match the tooth design |
| Suitable for a wide range of patients | Requires specific clinical conditions and greater prosthetic support |
| The traditional All-On-4 prosthetic format | Teeth appear to emerge directly from the gum |
Our Clinical Approach: Why We Prefer All-On-X for FP1 Cases
At Advanced Dental Artistry, when the clinical goal is an FP1 outcome, our preference is to use the All-On-X approach with six or more implants per arch rather than the standard four-implant protocol.
The reasoning is grounded in the specific demands of FP1 bridge design. An FP1 bridge sits directly against surgically contoured gum tissue with no pink material to bridge any gaps or compensate for minor positional variation. To achieve and maintain the precise fit that this design requires, the prosthetic bridge needs a higher density of implant support than is typically provided by four anchor points.
The Clinical Case for Additional Implants in FP1 Treatment
- Load distribution. With six or more implants, the forces of biting and chewing are spread across a greater number of anchor points. This reduces the mechanical stress on each individual implant and on the bone surrounding it.
- Prosthetic precision. A greater number of implants provides more reference points for the accurate positioning and seating of the bridge. In FP1 cases, where the fit between the bridge margin and the gum tissue is critical to the appearance of the result, this precision matters.
- Long-term bone preservation. Implants stimulate the surrounding jawbone through the transmission of functional forces, which helps maintain bone volume over time. A higher density of implants distributes this stimulation more evenly across the arch.
- Stability of the gum contour. The surgical shaping of the gum tissue in FP1 cases creates a specific contour that the bridge is designed to follow. Maintaining that contour over the long term is supported by a stable, well-supported prosthetic platform.
It is important to note that the number of implants appropriate for any individual patient is determined by a detailed clinical assessment, including three-dimensional imaging of the jawbone. The decision is made on clinical grounds and in discussion with the patient, not as a blanket protocol applied to all cases.
All-On-4 vs All-On-X: A Side-by-Side Comparison
| All-On-4 | All-On-X (6+ Implants) | |
| Number of implants | Fixed: 4 per arch | Variable: typically 6 or more per arch |
| Protocol type | Standardised | Individualised based on clinical assessment |
| Prosthetic options | Primarily FP3 | FP3 or FP1, depending on case suitability |
| FP1 bridge suitability | Limited by implant density | Supported by higher implant density |
| Load distribution | Across 4 anchor points | Across 6 or more anchor points |
| Bone grafting (typical) | Often avoidable | Depends on individual bone assessment |
| Gum sculpting (FP1 cases) | Not typically indicated | Surgical gum contouring performed |
| Best suited to | Patients seeking a fixed, well-established solution with sufficient bone for 4 implants | Patients seeking FP1 outcomes or those with anatomy or clinical goals suited to additional implant support |
Patient Suitability: What Determines the Right Approach?
The choice between All-On-4 and All-On-X is not one patients make independently. It is the outcome of a detailed clinical assessment that takes into account a range of individual factors. Some of the key considerations include:
Bone Volume and Density
The volume and density of bone available in the jaw is a primary factor in implant treatment planning. Three-dimensional imaging (CBCT scanning) allows the treating dentist to assess the precise dimensions and quality of available bone at each potential implant site. This assessment informs both the number of implants that can be placed and their optimal positions.
Prosthetic Goals
The type of bridge a patient is seeking, specifically whether the goal is an FP3 or FP1 outcome, is a significant factor in determining the appropriate number of implants. Patients who are interested in an FP1 result will typically be assessed for suitability for the All-On-X approach, given the clinical support requirements described above.
Overall Oral and General Health
Medical history, current medications, and overall oral health all play a role in treatment planning for full arch implant cases. Conditions such as uncontrolled diabetes, the use of bisphosphonate medications (a class of drug commonly prescribed for osteoporosis and certain bone conditions), and active gum disease are among the factors that a treating dentist will evaluate prior to recommending a treatment pathway.
Existing Bone Loss and Gum Tissue
In FP1 cases, the volume and health of gum tissue is particularly relevant. Surgical gum contouring is performed to create the scalloped tissue architecture that allows the FP1 bridge to sit naturally at the gum line. The suitability of the existing gum tissue for this shaping procedure is assessed during the clinical planning phase.
Not every patient is a suitable candidate for full arch implant treatment, and not every patient who is suitable for All-On-4 is necessarily a candidate for All-On-X or FP1 outcomes. Suitability is determined through a thorough clinical assessment, not by general interest in a particular approach. The information in this guide is provided as educational background to help patients ask informed questions at their consultation.
Clinical Advantages of a Higher Implant Count in Full Arch Cases
Where clinical assessment indicates that six or more implants per arch are appropriate, there are several established clinical rationales that support this approach.
- Broader load distribution. The forces generated during chewing are distributed across a greater number of implant-bone interfaces, reducing peak stress at any individual site.
- Enhanced long-term stability. A greater number of implants can provide a more stable prosthetic platform, which may support the longevity of both the implants and the bridge over time. Individual outcomes will depend on a range of clinical factors including bone quality, oral hygiene, and follow-up care.
- Bone stimulation across a wider arch area. Implants transmit functional forces into the surrounding bone, which supports bone maintenance. A higher implant count distributes this stimulation more broadly along the arch.
- Greater prosthetic precision. For bridge designs that require close adaptation to the gum tissue, as in FP1 cases, more anchor points allow for more precise positioning and a more stable fit over time.
Summary: Key Differences Between All-On-4 and All-On-X
- All-On-4 uses a fixed protocol of four implants per arch. It is a well-established approach suitable for many patients seeking fixed full arch replacement.
- All-On-X uses a variable number of implants, typically six or more, determined by individual clinical assessment. It is not a single protocol but a flexible framework.
- The two approaches are most meaningfully differentiated by the prosthetic outcomes they support. All-On-4 is most closely associated with FP3 bridge designs. All-On-X is the approach used when an FP1 outcome is the clinical goal.
- FP3 bridges replace teeth and simulated gum tissue. FP1 bridges attach directly to surgically contoured natural gum tissue, with teeth appearing to emerge from the gum line.
- At Advanced Dental Artistry, the preference for All-On-X in FP1 cases reflects the higher level of prosthetic support required to achieve and maintain the precise fit that direct-to-gum bridge design demands.
- Determining which approach is appropriate requires a thorough clinical assessment. Patient interest in a particular outcome is the starting point, not the endpoint, of the planning process.
Considering Full Arch Implant Treatment? Begin With a Consultation
Understanding the clinical differences between All-On-4 and All-On-X, including the role of prosthetic classification in determining the right approach, is best followed by a conversation with a treating dentist who can assess your individual situation. At Advanced Dental Artistry in West Perth, we focus exclusively on dental implants, All-On-4/All-On-X full arch replacement, and veneers. We welcome patients at any stage of their research, including those who simply have questions they would like answered before making any decisions.
Call us to speak with our team | Book a consultation online | Visit us at 555 Newcastle Street, West Perth